Rehabilitation tries to address morbidities and their consequences through education and exercise. Patients are encouraged to become more actively involved in their own health care, more independent in ADLs and less dependent on health professionals and expensive medical resources. Rather than focusing solely on reversing disease processes, rehab attempts to reduce symptoms and make individual more functional
Purpose
Restore function following an illness or injury, with the goal of maximizing a person’s ability to achieve fullest life possible
Who can benefit?
Chronic respiratory disease symptomatic with optimum drug therapy
Chronic cardiovascular diseases with breathlessness despite optimum intervention and drug therapy
Chronic neurological diseases
Chronic orthopaedic diseases& post operative
Lifestyle disoders like Stress,Sleep , Obesity
Special children
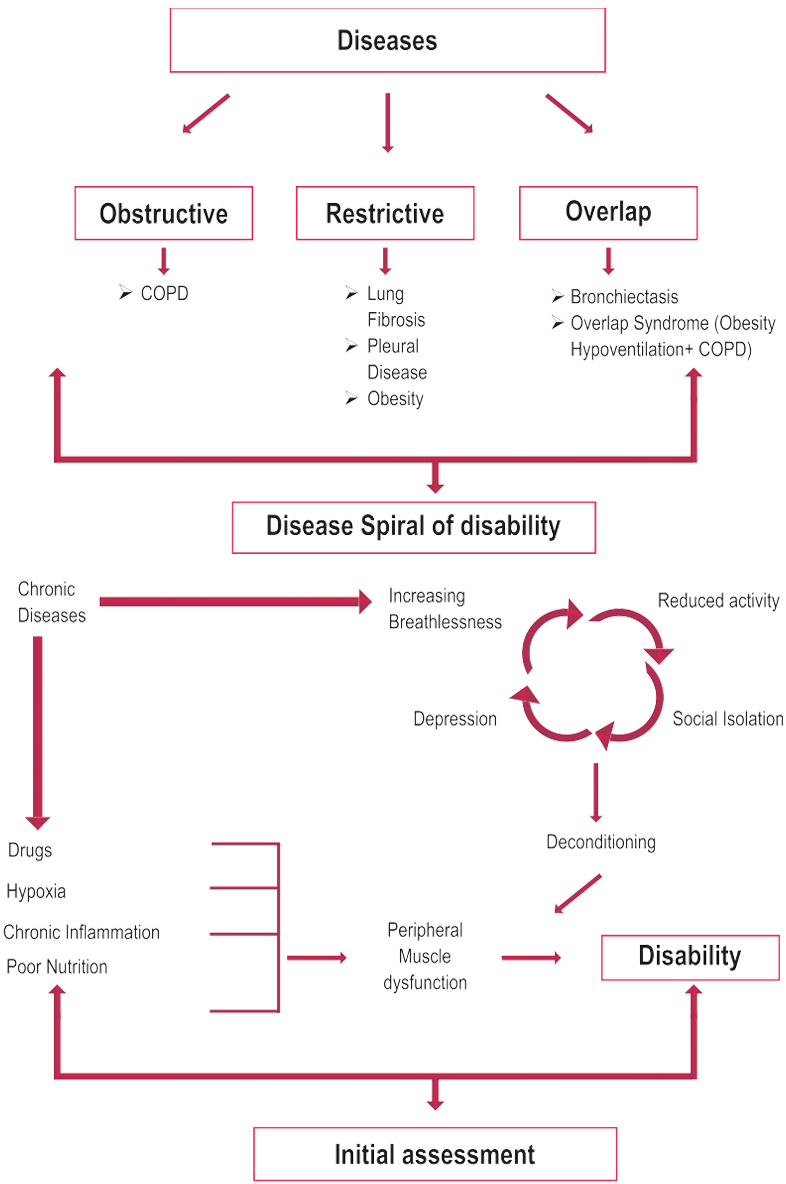
Consequences of advanced chronic diseases
Peripheral Muscle dysfunction
Respiratory muscle dysfunction
Nutritional abnormalities
Cardiac impairment
Skeletal disease
Sensory defects
Neuro cognitive dysfunction
Psychosocial dysfunction
Mechanisms for these morbidities
Deconditioning
Malnutrition
Effects of hypoxemia
Steroid myopathy
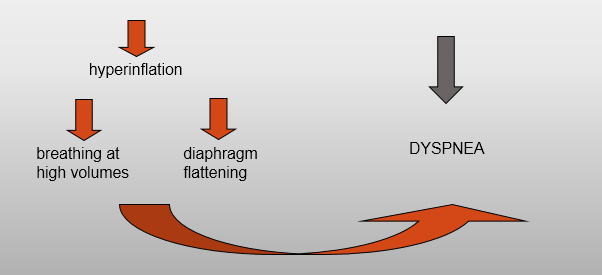
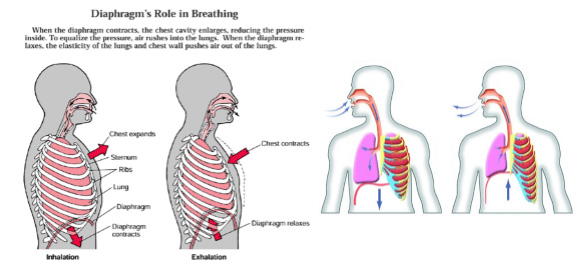
Hyperinflation
Diaphragmatic fatigue
Psychosocial dysfunction from anxiety, guilt, dependency and sleep disturbances.
Benefits
Improved Exercise Capacity
Reduced perceived intensity of dyspnea
Improve health-related QOL
Reduced hospitalization
Reduced anxiety and depression
Improved limb function
Benefits extend well beyond immediate period of training.
Psychosocial dysfunction from anxiety, guilt, dependency and sleep disturbances.
Pulmonary Rehabilitation
“A multidisciplinary continuum of services directed to persons with pulmonary diseases and their families, usually by an interdisciplinary team of specialists, with the goal of achieving and maintaining the individual’s maximum level of independence and functioning in the community”
Benefits of Pulmonary Rehab.
The benefits are seen in irreversible pulmonary disorders because much of the disability is not from the lung disease but from the secondary morbidities.
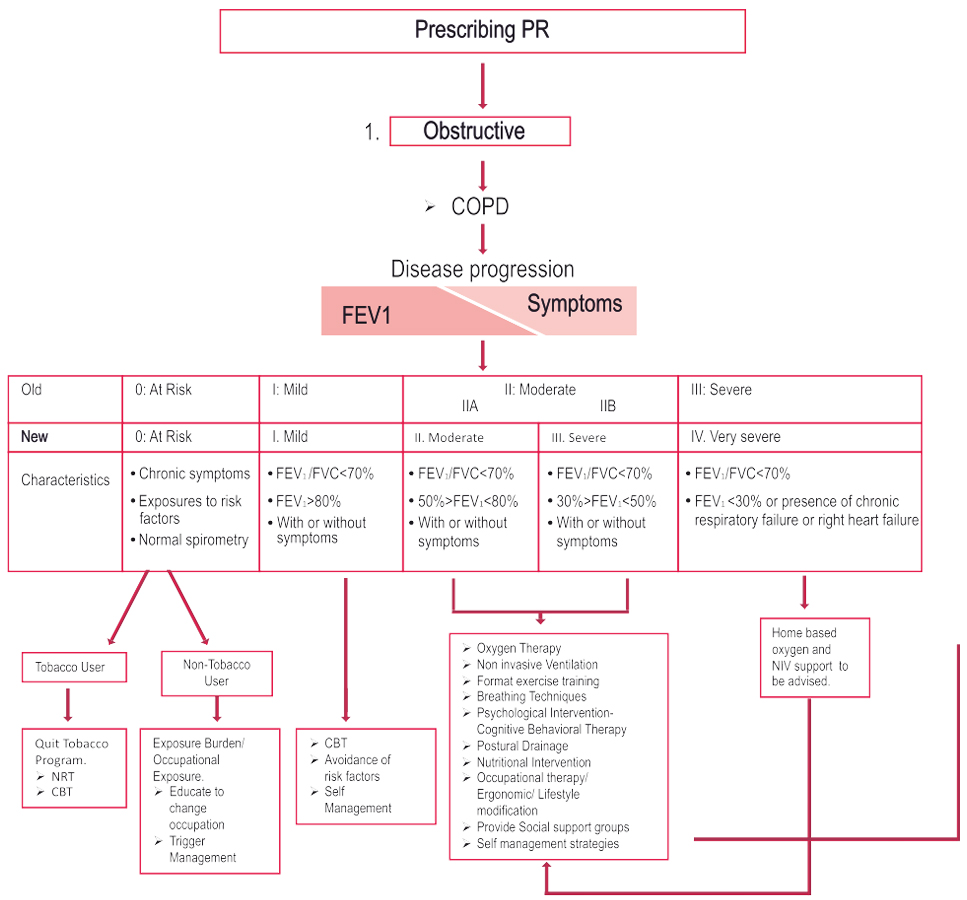
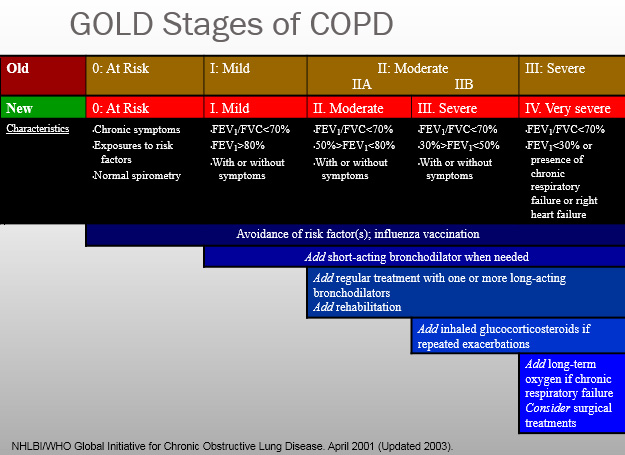
Objective Abnormalities
FEV1 less than 80% predicted
FEV1/FVC less than 70 %
DLCO less than or equal to 65% of predicted
Resting hypoxemia less than or equal to 90%
Exercise Testing demonstrating hypoxemia less than 90%
Enrolling active smokers is controversial but they may benefit significantly with a focus on smoking cessation.
Patient Motivation is a necessary consideration.
Setting for Pulmonary Rehabilitation
Outpatient
Inpatient
Home
Community Based
Choice varies depending on
Distance to program
Insurance payer coverage
Patient preference
Physical, functional, psychosocial status of patient
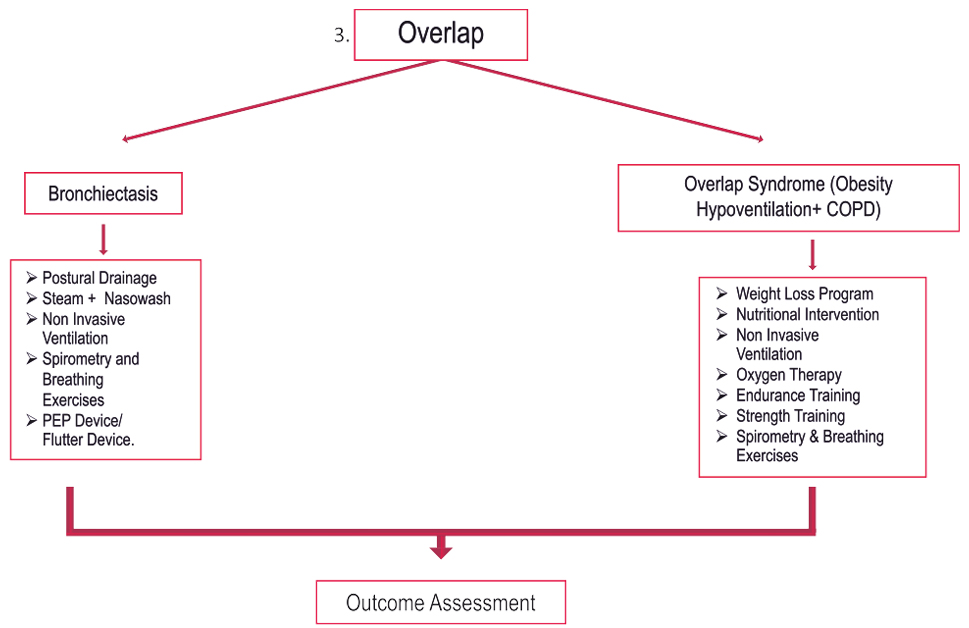
Diaphragm Breathing – Some patients with extreme air trapping and hyperinflation have increased WOB with this technique
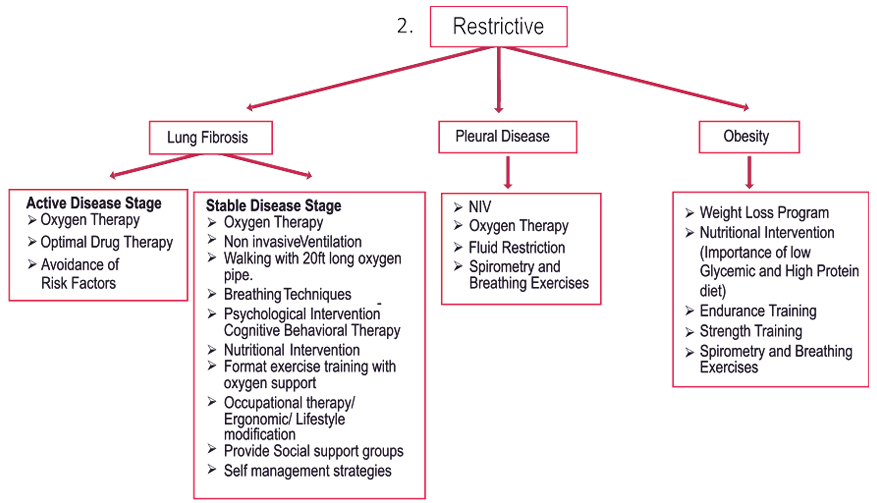
Postural Draining – valuable in patients who produce more than 30cc/24 hours/ Coughing techniques
Nutritional Assessment
Diet history, BMI
Over or Under weight.
Classes in weight management and/or nutritional counseling to improve weight management
Outcome Assessment
An important component of pulmonary rehabilitation, being used to determine individual patient responses and evaluate overall effectiveness of program.
Dyspnea 10 pt scale, Borg scale, Visual Analog Scale
Exercise Ability – Borg Scale, 6MDW/Progressive exercise testing pre and post rehab.
Health Status – Respiratory-related QOL; CRDQ
Activity Levels –Respiratory-Specific functional Status, Duke Functional Status Scale.