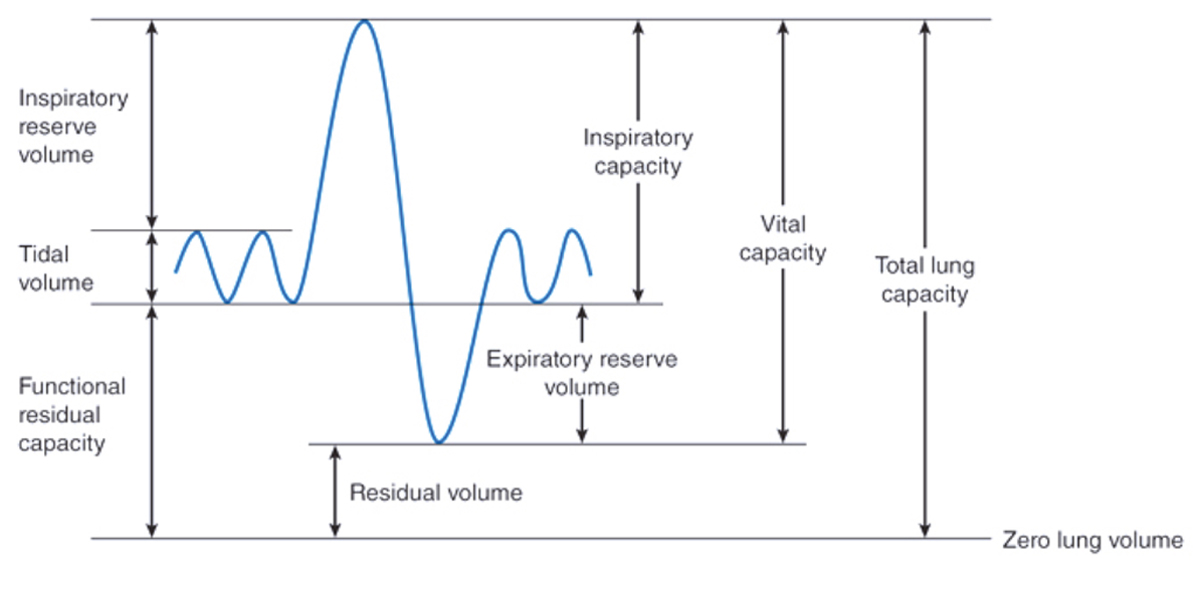
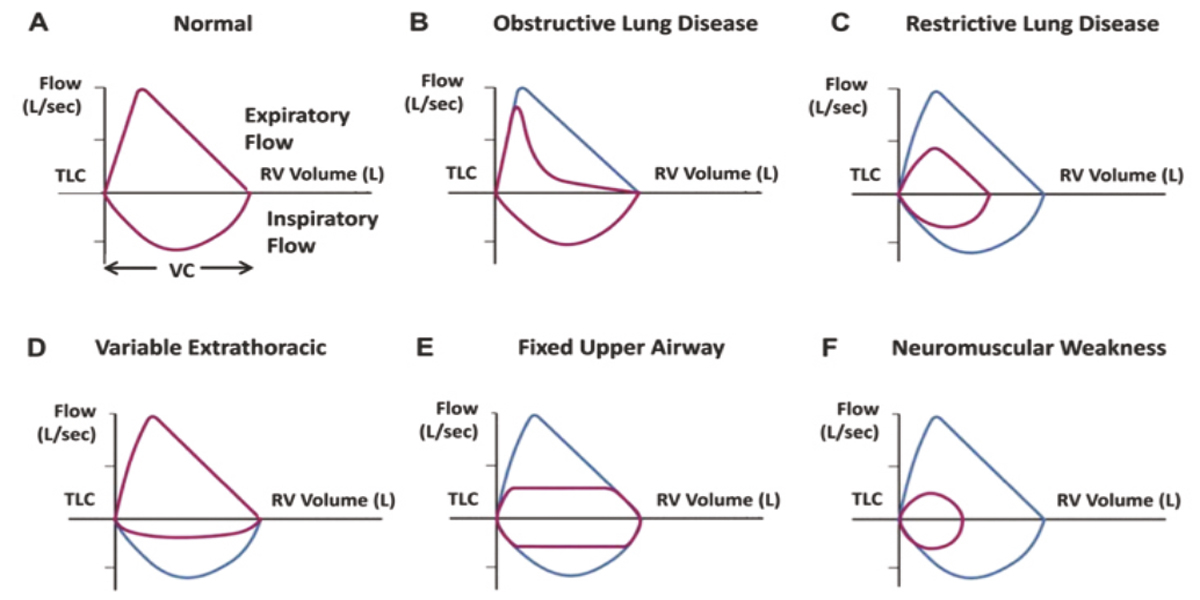
There are two main ventilatory patterns measured by pulmonary function tests: obstruction and restriction. Categorization of these patterns is dictated by the lung volumes, both static and forced, as well as the interpretation of the flow-volume loop.
Minimal recommendations for spirometry systems: The spirometer equipment must be able to accommodate a volume of atleast 8 liters, accumulating continuously for minimum 15 seconds at airflow rate between 0-14L/s. The total resistance to airflow t 14.0 Lismustbe <1.5cmH20/L/s
Spirometry may indicate the presence or absence of Restrictive lung disease which can be confirmed by measuring lung volumesin advance pulmonary function tests,
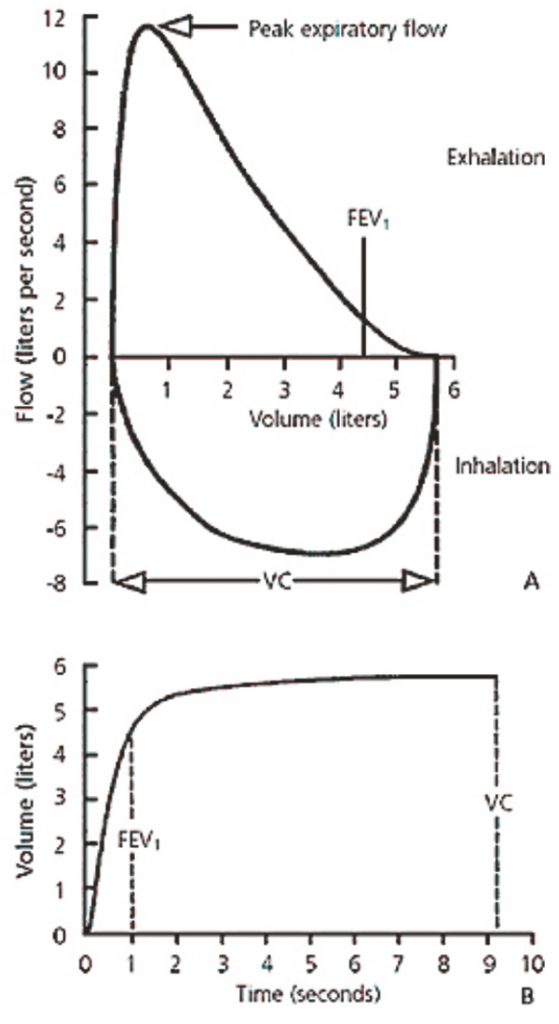
Severity: Severity assessment of both restrictive and obstructive defects on spirometry should be based on FEV! values Severity can be categorized as mild, moderate, and severe when FEV’1(Pre for asthma and post for COPD) is 270%, 50%-69%, and <50% predicted, respectively.
Because pulmonary function testing is effort dependent, technicians must be trained sufficiently and laboratories mustadhere to high standards to obtain the most accurate and reproducible results possible
Measurements from spirometry alone can be useful in patients whose main physiologic impairment is airway obstruction. The findings from spirometry can provide clues that concomitant restriction is present; however, forassessmentof restriction, lung volumes mustbe measured.
In patients with reversible mild airway disease, the results of pulmonary function tests may be normal because the disease is dynamic and patients with mild.irflow obstruction may spontaneously return to normal.
Thediffusing capacity measurementis used to determine defects ofthe alveolar-pulmonary capillary unit. Adefectin the diffusing capacity alerts the physician that oxygen transfer, the alveotar-capillary membranes, and/or pulmonary capillaries may not be normal, and further evaluation ofthe underlying cause of this defect should be pursued,
Methacholine provocation testing is used to identify whether abnormal airway responsiveness is present. Usually this indicates a diagnosis of asthma, but the clinician must understand that other conditions that involve airway inflammation, such as sarcoidosis, may also show abnormal airway responsiveness.

{kind=link}